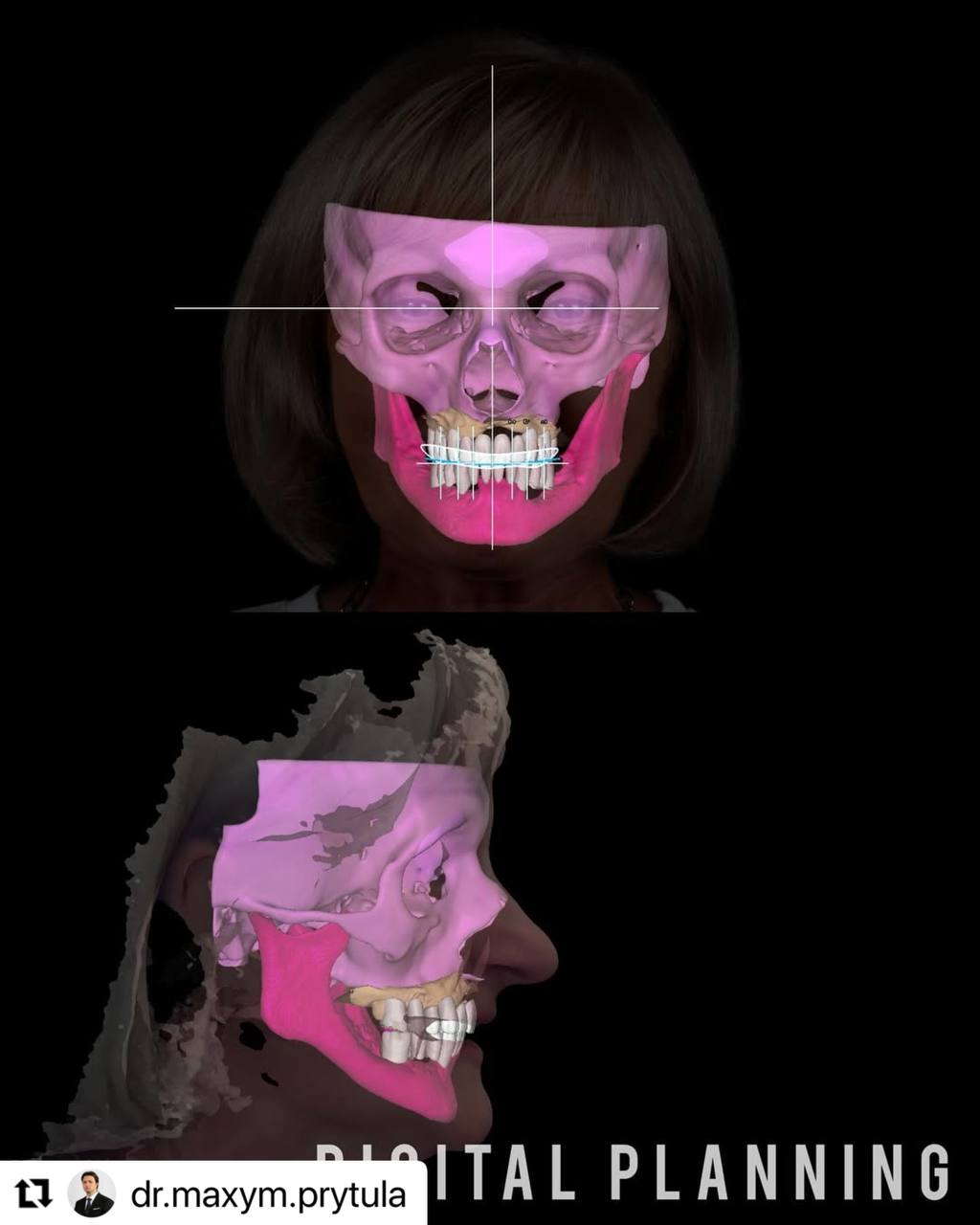
An interesting case illustrating the ability to combine different approaches and implant configurations depending on the atrophy of the maxilla.

Residual bone and anchorage points are a hot topic of discussion at the moment, due to different schools clashing on what approach is more stable: a 10- mm tilted palataly exposed implant or a 30+ mm zygomatic implant. In this specific clinical case we had the opportunity to properly utilise both techniques in respect to the indications for them.
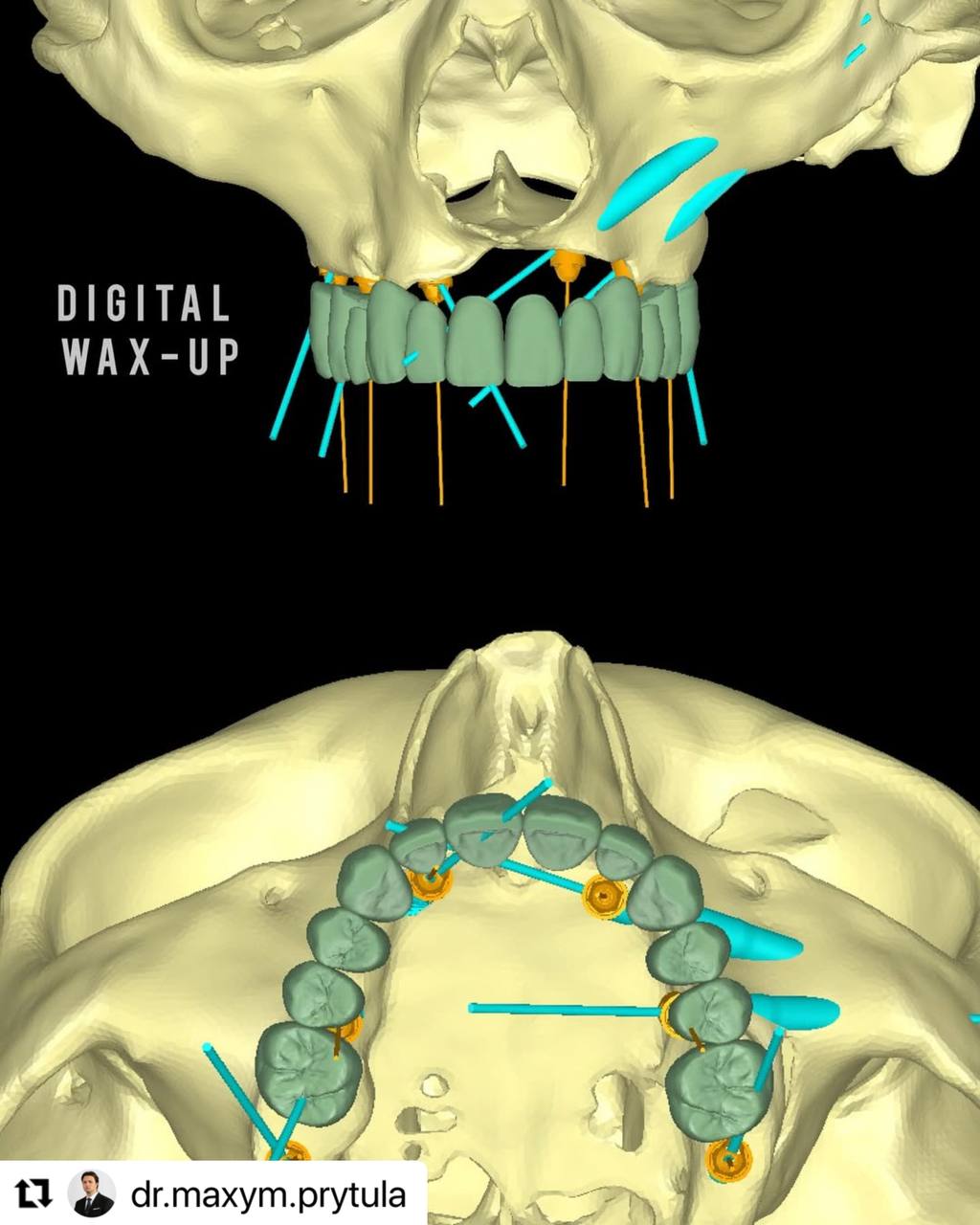
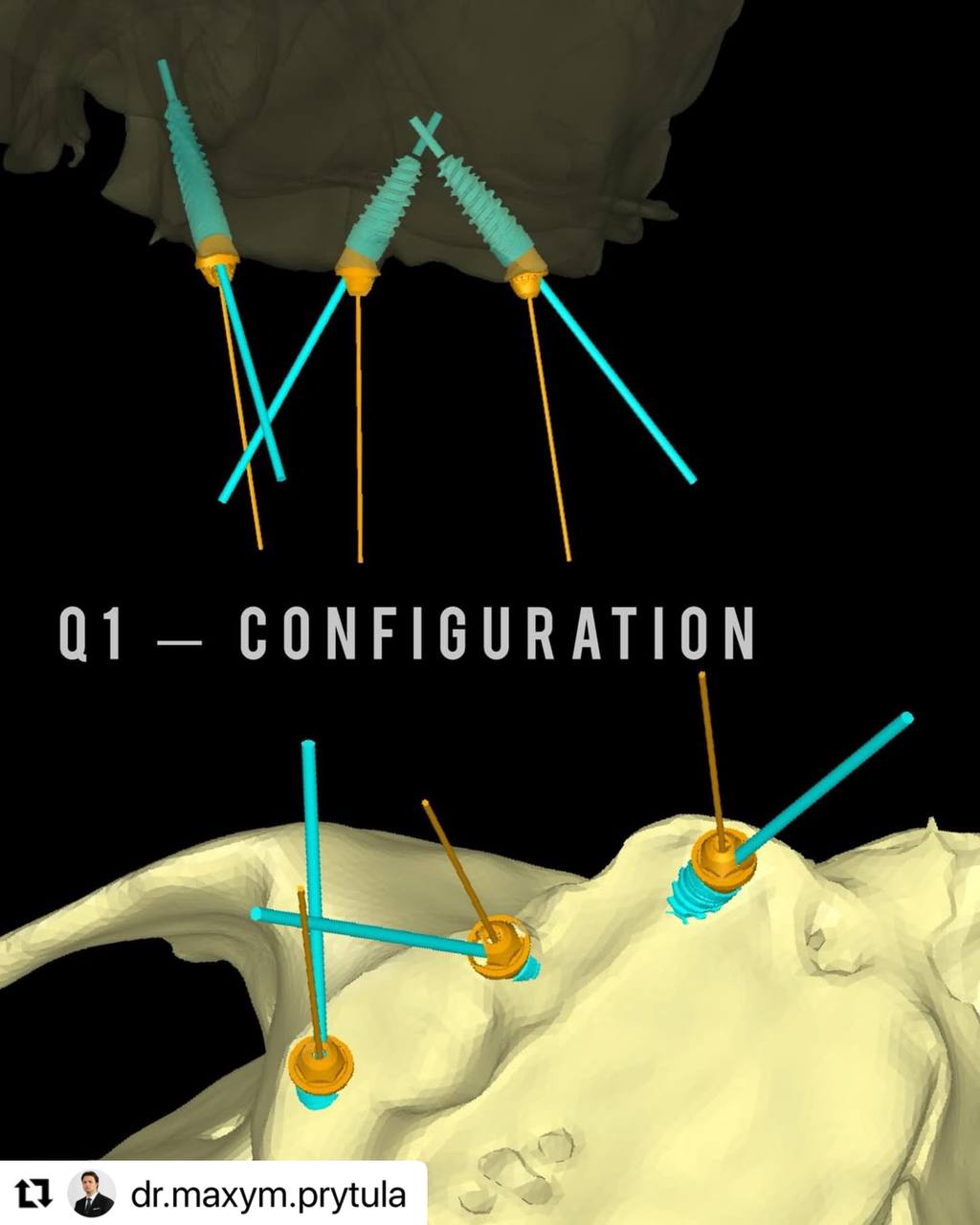
The first sector while being both vertically and horizontally atrophied had enough bone proposition to place a 11.5mm anterior palatally-exposed implant into the canine pillar and a 13mm tilted implant in Zone2.
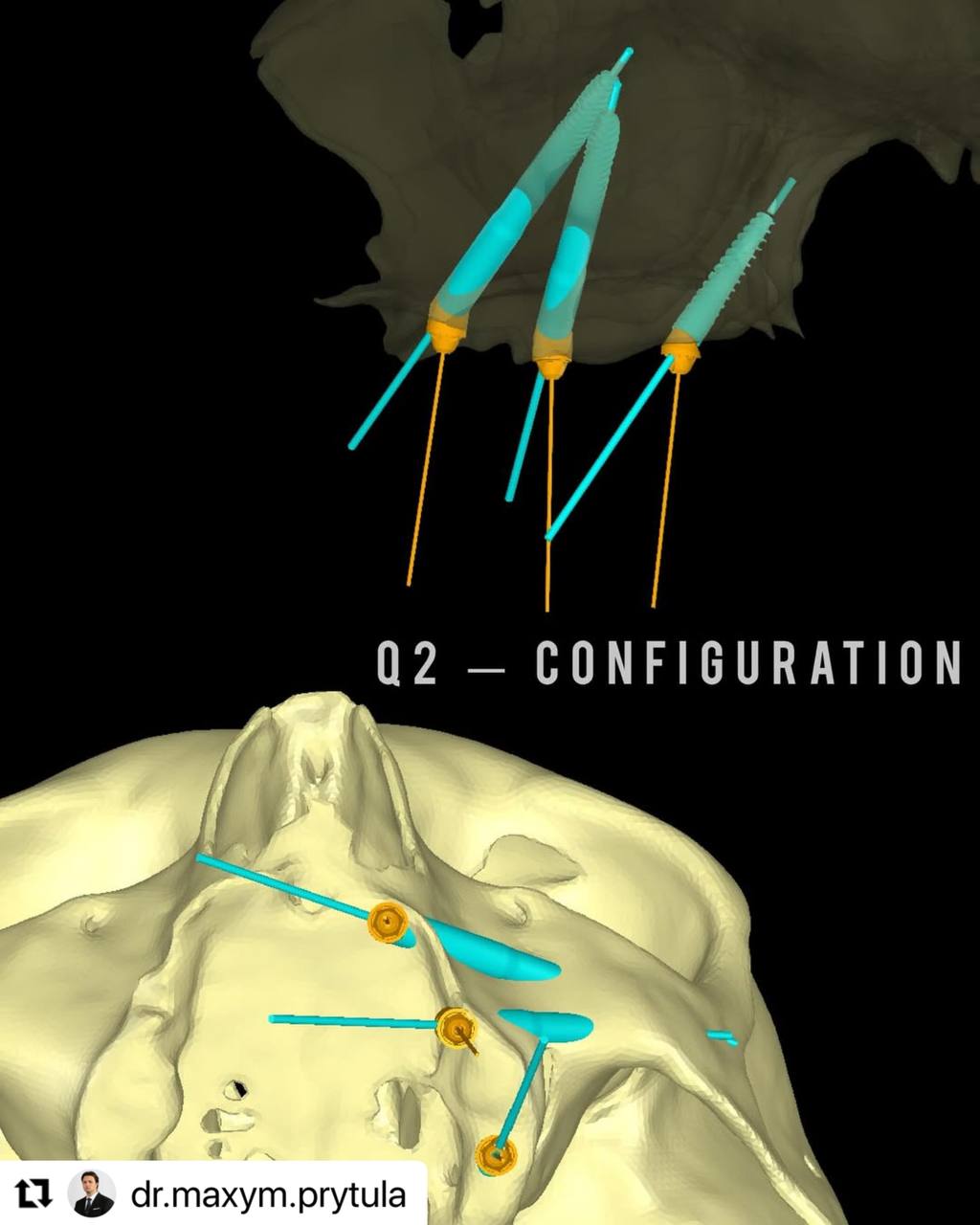
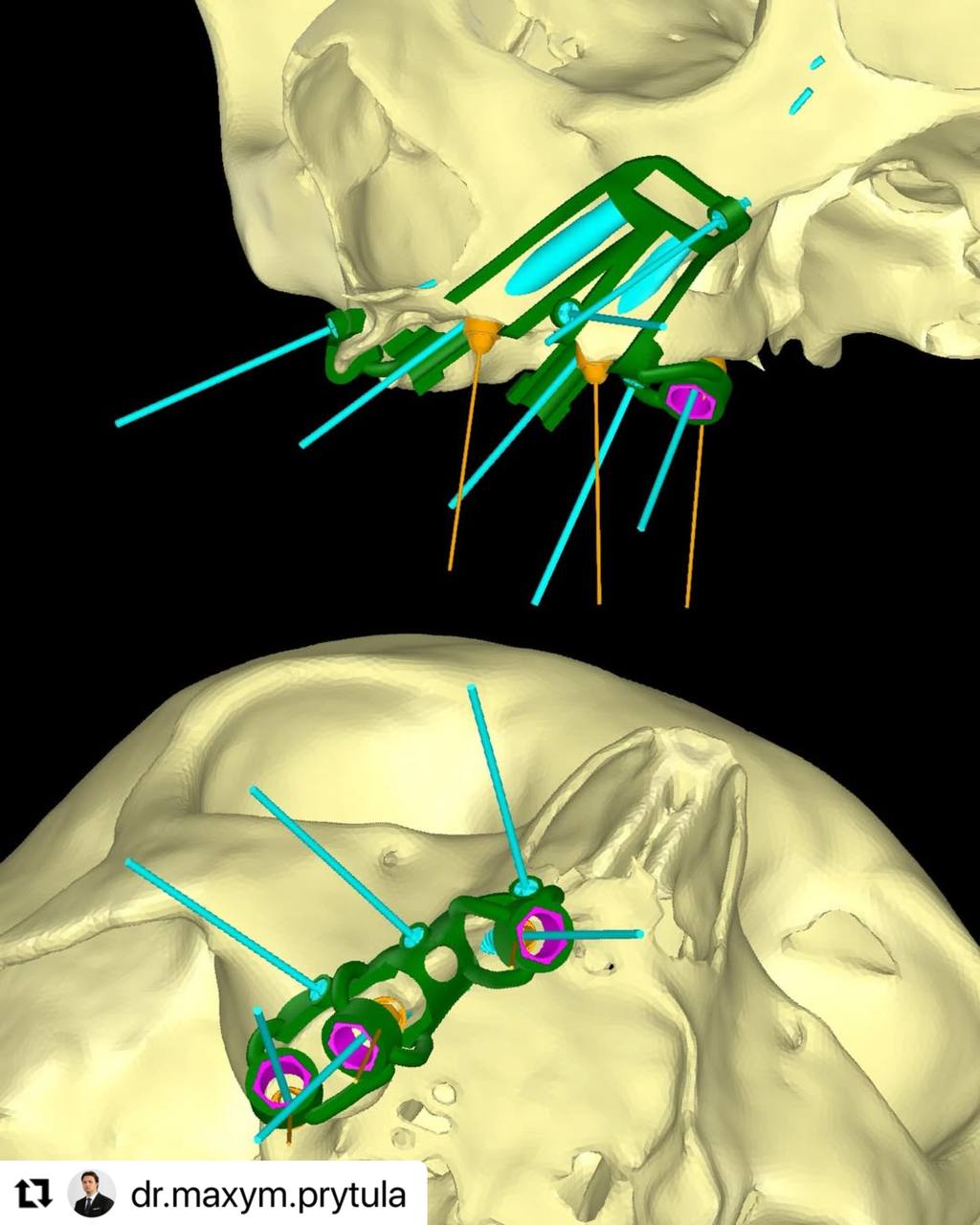
The second sector however did not have any residual bone whatsoever , including the absence of the Z-point hence the double-Zygoma configuration.

While I find anterior zygomatic implants a defective technique from a biomechanical perspective in comparison to conventional and trans-nasal implants it is important to note that no alternative was available in this specific situation.


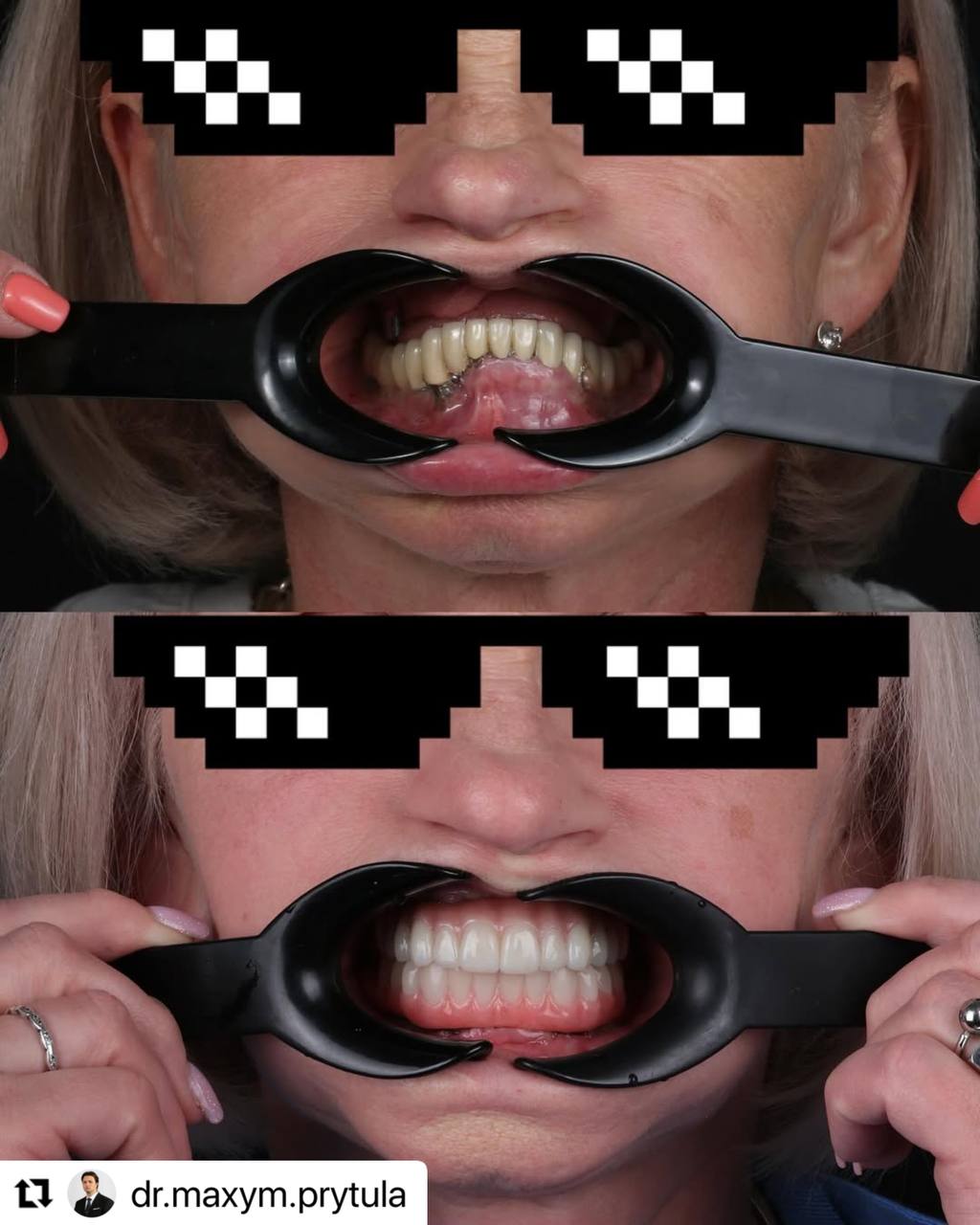
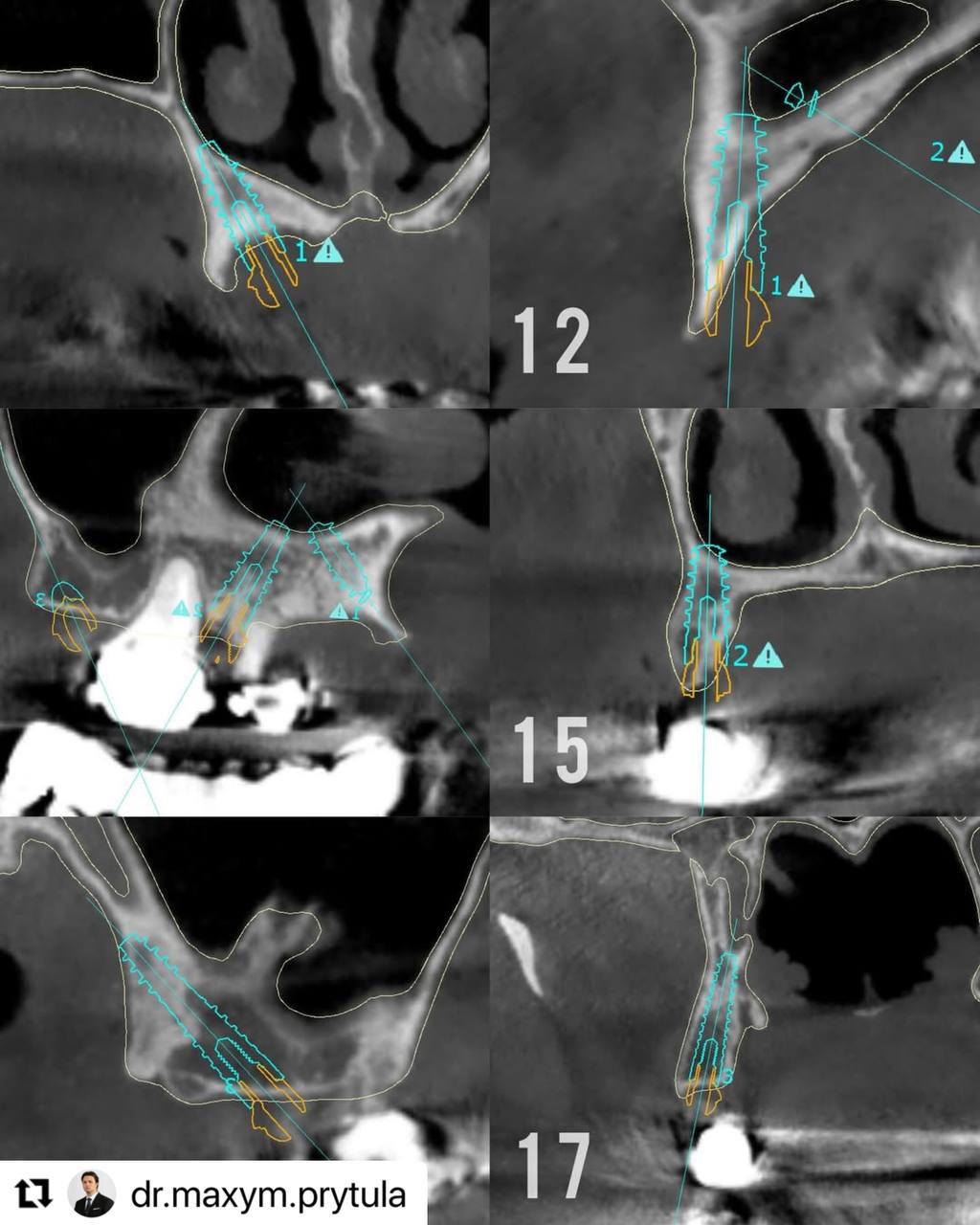
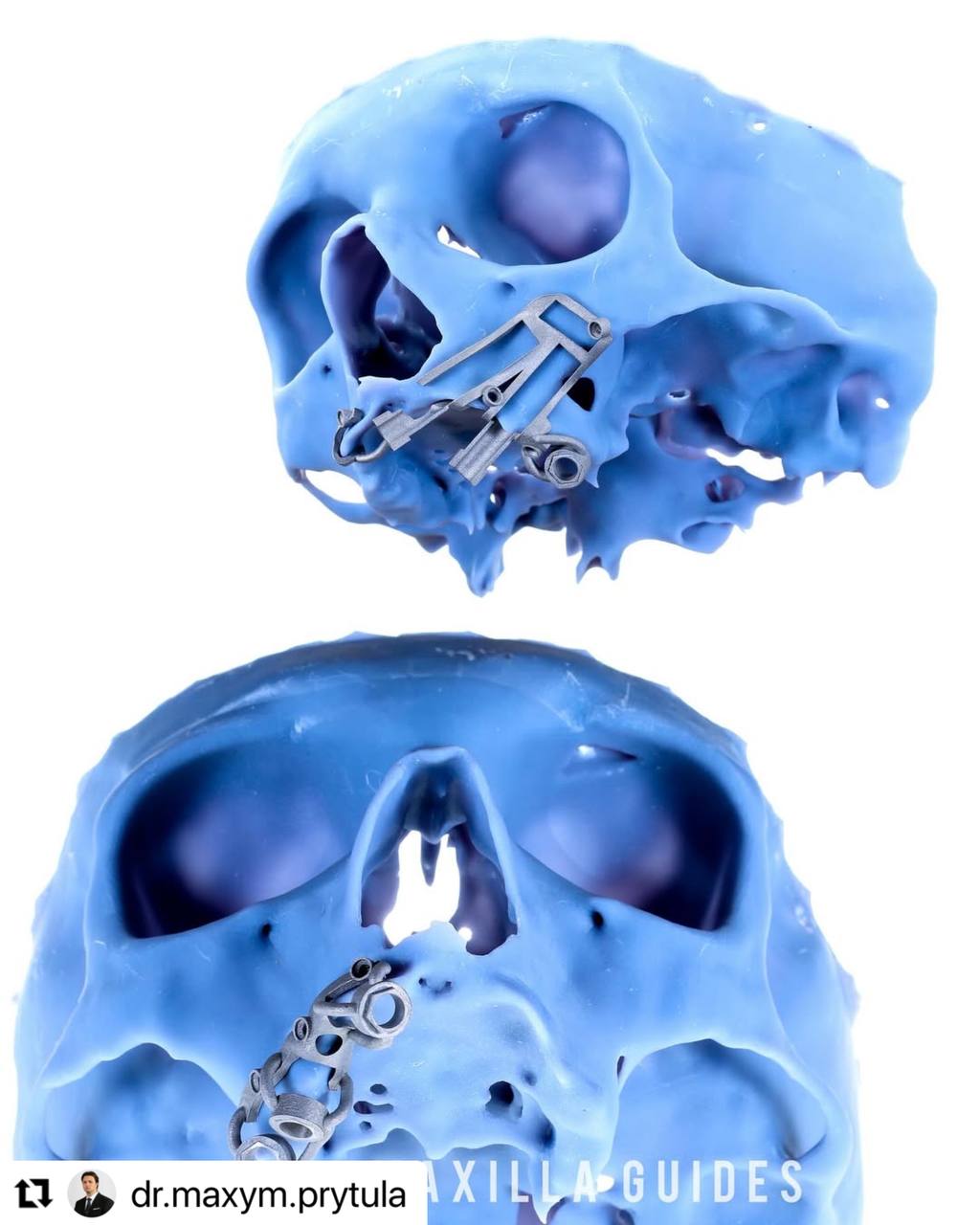
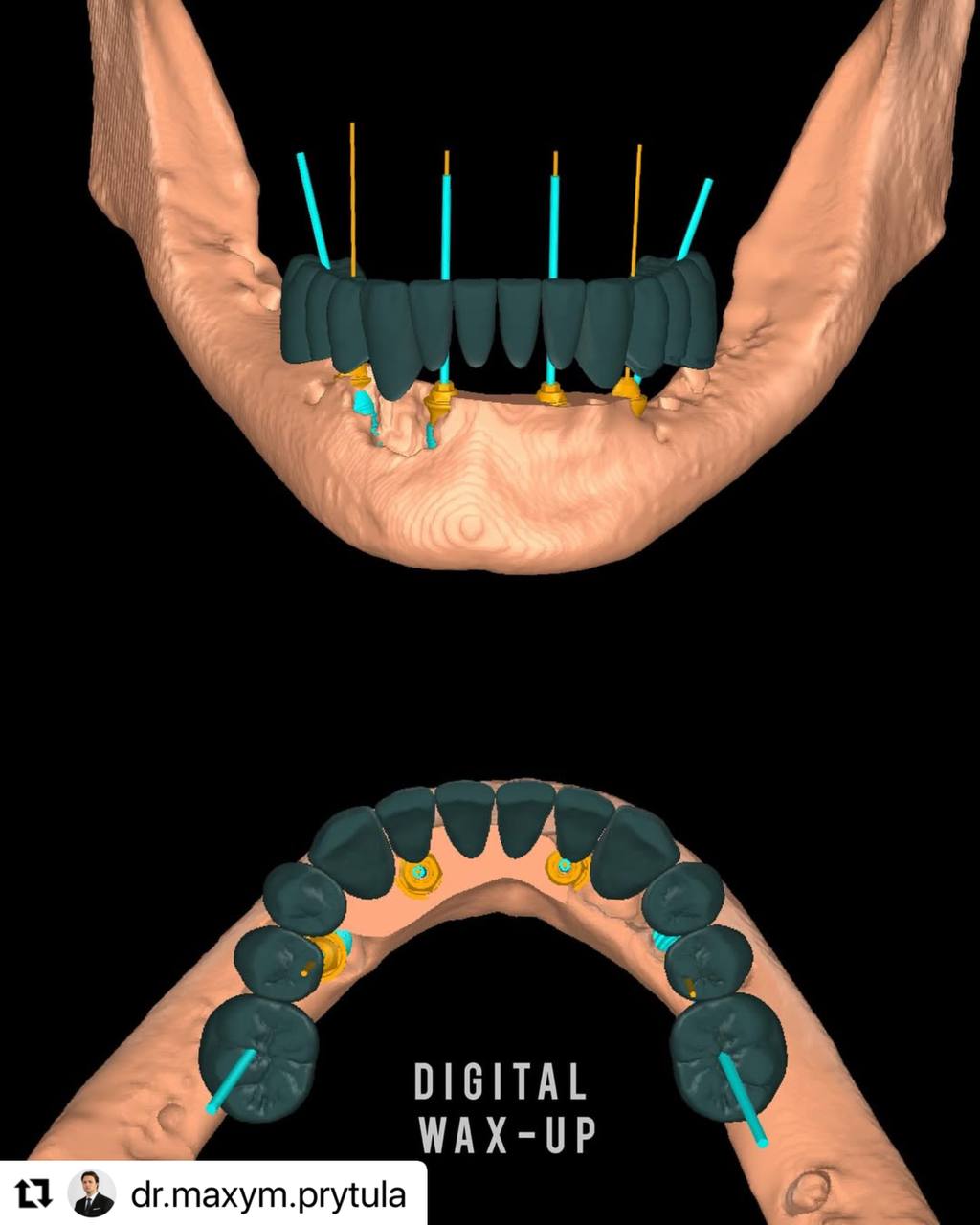
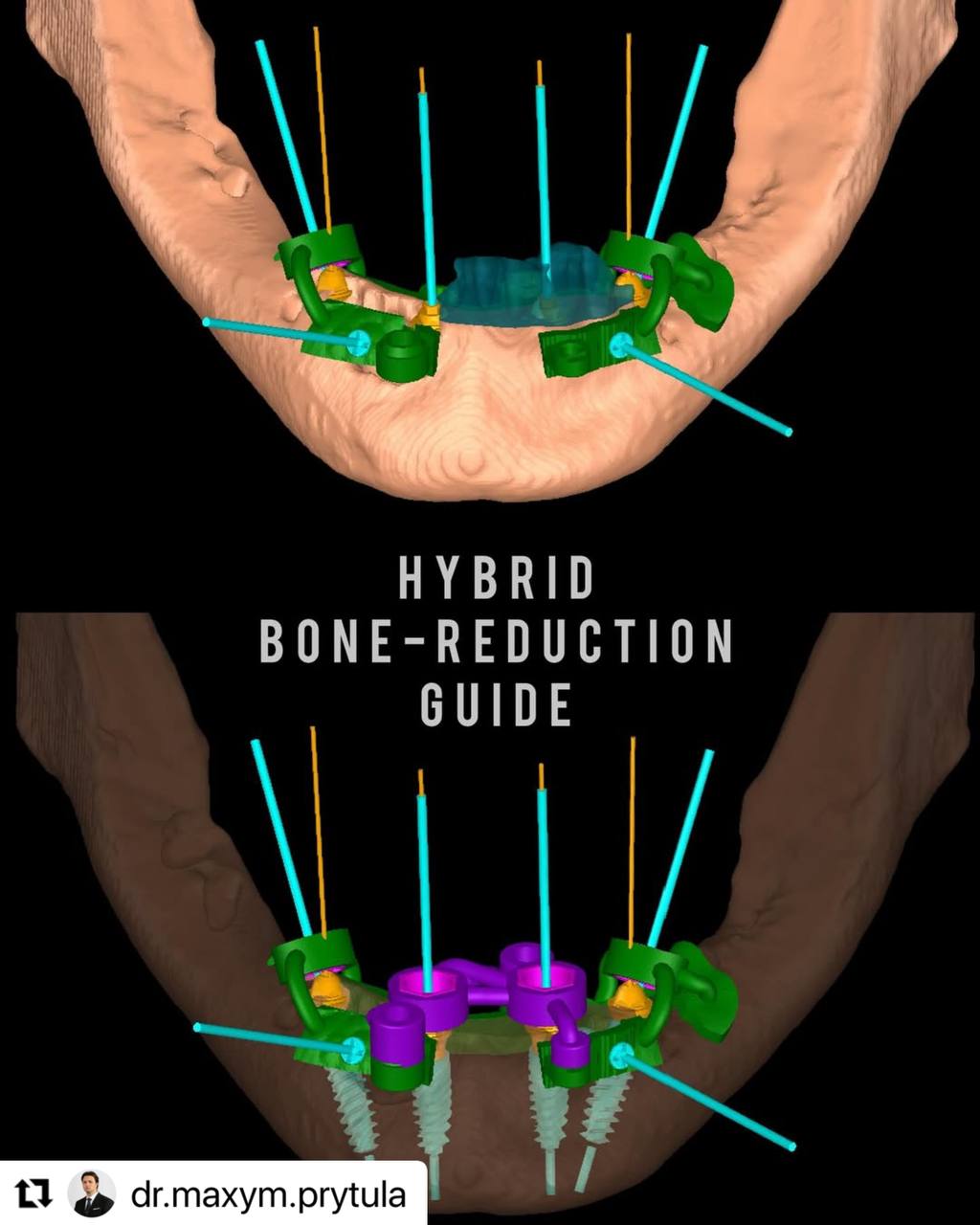
In these scenarios anatomical precision is a key factor, that is why we tend to utilise guided surgery, mainly bone-supported guides, which allow us to confidently place implants and achieve high primary stability while at the same time providing an optimal restorative position to better distribute AP-spread. Overall, both approaches are effective and allow the patient to be loaded immediately and receive a final prosthesis in 3-4 months, however indications have to be respected.
Case by Dr. Prytula and Dr. Beygul
TO ALL ARTICLES